

Summary
When navigating the complexities of HSV-1 vs HSV-2 dating, the first question you’ll often hear — from your doctor, from online forums, or from your own anxious 2 a.m. search history — is: which type do you have? The answer matters more than people usually explain. It’s not just a medical distinction; it has practical implications for your dating life, the specific conversations you’ll have with a new partner, your need for daily medication, and your overall understanding of what you’re living with. This article breaks down those differences in terms that are actually useful to you.
- The Global Reality: HSV-1 vs HSV-2 Dating by the Numbers
- Recurrence Rates and What They Mean Day-to-Day
- Asymptomatic Shedding: The Number That Changes the Transmission Conversation
- The Stigma Gap — and Why It Makes No Medical Sense
- Does Your Type Change How You Disclose?
- Suppressive Therapy: Who Actually Needs It?
- Side-by-Side Comparison
- Frequently Asked Questions
The Global Reality: HSV-1 vs HSV-2 Dating by the Numbers
Before diving into the clinical differences, it helps to understand the sheer scale of both types. When you realize how many people are in the same boat, it completely reframes the HSV-1 vs HSV-2 dating landscape.
Global Prevalence at a Glance
(Data based on WHO & STI Journal, 2020-2025 estimates)
| Infection Type | Estimated Global Population (Ages 15–49) | Key Takeaway |
| HSV-1 (Any site) | 3.8 Billion (64%) | Mostly oral infections acquired in childhood. |
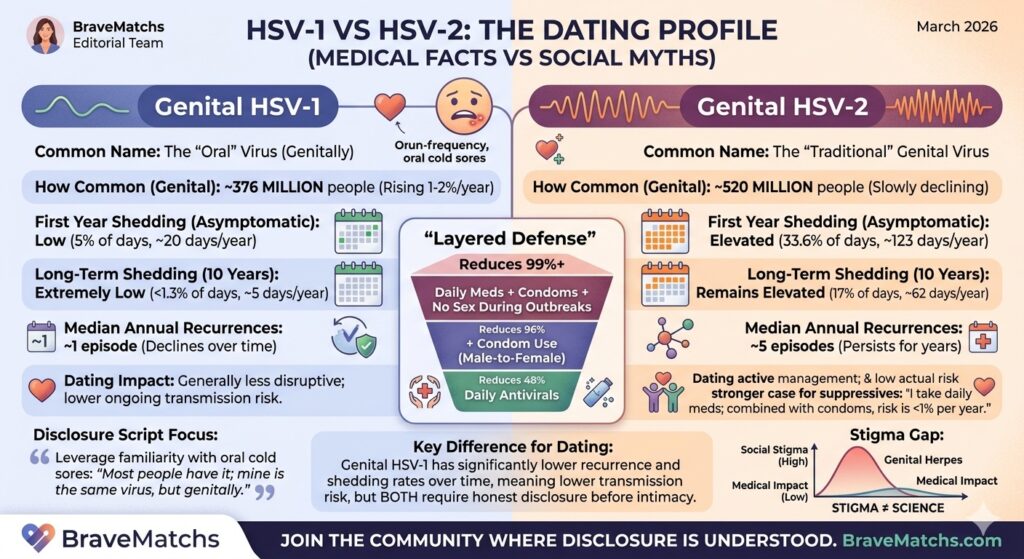
| Genital HSV-1 | 376 Million (10%) | Rising by 1–2% annually in high-income countries. |
| Genital HSV-2 | 520 Million (13%) | Slowly declining, but still the most common genital type. |
| Combined Genital | 846 Million (20%+) | More than 1 in 5 adults live with genital herpes. |
The Reality of Your Dating Pool
The implications of these numbers are worth sitting with:
Oral HSV-1 is Everywhere: Most people you meet already carry HSV-1 orally, whether they know it or not.
The “1 in 5” Rule: In any room of adults, a significant portion is living with some form of genital herpes.
Rising Genital HSV-1: As sexual practices change, genital HSV-1 is becoming increasingly common, partially filling the gap as HSV-2 rates dip.
The silence surrounding herpes is dramatically out of proportion to how common it actually is. Whether a partner has a diagnosis or not, there is a meaningful chance they are already part of these statistics.
Recurrence Rates — The Number That Changes Your Daily Life
This is where HSV-1 and HSV-2 diverge most clearly, and where the difference has the most practical impact on your dating life.
Genital HSV-2: Frequent and Persistent
People with genital HSV-2 experience a median of five symptomatic recurrences per year after the initial episode — though this varies significantly from person to person. Nearly all people with symptomatic first-episode HSV-2 go on to have recurrent episodes at some point. Recurrence frequency tends to decrease over time, but roughly one in four people actually sees an increase in recurrence rates five years after initial infection.
For dating, this means HSV-2 is something you’ll be managing more actively and consistently. Outbreaks can affect intimacy timing, create anxiety in new relationships, and require more ongoing communication with a partner.
Genital HSV-1: Lower and Declining
Genital HSV-1 behaves quite differently. Clinical data show a median of one symptomatic recurrence in the first year after initial infection — and recurrence rates continue to fall after that. Around 30% of people with genital HSV-1 experience no recurrence at all in the first year. This is because HSV-1, which evolved to live in the trigeminal ganglia (near the face), is less efficient at reactivating from the sacral ganglia where genital infections are established.
For dating, this means genital HSV-1 tends to be less disruptive to everyday life and intimacy than genital HSV-2. It doesn’t make it less real — the disclosure conversation still matters — but the ongoing management is generally less demanding.
Asymptomatic Shedding — The Transmission Conversation
Asymptomatic shedding is what makes herpes transmissible even when there are no visible symptoms — no outbreak, no warning, nothing to see. It’s the reason disclosure matters regardless of whether you “feel fine.” And it’s where HSV-1 and HSV-2 differ most dramatically in terms of ongoing transmission risk.
A landmark study from the University of Washington, published in JAMA in 2022 (Johnston, Magaret et al.), tracked genital viral shedding in people with first-episode genital HSV-1 for a full year. The findings were significant:
- Genital HSV-1 shedding occurred on approximately 5% of days in the first year — and in the subset who continued to shed beyond month 11, rates had fallen to just 1.3% of days by year three.
- Genital HSV-2 shedding, by comparison, occurs on approximately 33.6% of days in the first year after infection — and remains elevated at 17% of days even 10 years later.
To put that in plain terms: someone with genital HSV-2 who has had the infection for a decade is still shedding virus on roughly one in six days with no symptoms. Someone with genital HSV-1 is shedding on a small fraction of days, with rates that continue to fall over time.
This difference in shedding — not just outbreak frequency — is why the transmission risk profile of genital HSV-1 and HSV-2 is meaningfully different, and why the conversation you have with a new partner can legitimately include different information depending on which type you have.
That said: both types shed asymptomatically. Both can be transmitted without symptoms. Both require the same disclosure conversation. Lower risk is not zero risk, and knowing your shedding profile doesn’t change your ethical or legal obligations to a partner. It does, however, give you accurate information to share — which is always better than silence.
The Stigma Gap — and Why It Makes No Medical Sense
Here’s something worth saying plainly: the social stigma attached to herpes bears almost no relationship to the actual medical or scientific reality of either type.
Most people’s first reaction to hearing “I have cold sores” — oral HSV-1 — is to shrug it off as a minor, common, unremarkable thing. And statistically, they’re right: the majority of adults carry it. But the moment “genital” enters the picture, the same virus — or its close relative — suddenly becomes freighted with shame, judgment, and fear that the medical facts simply don’t support.
This stigma gap creates a strange situation in the dating world. Someone with oral HSV-1 who transmits it through kissing to a partner — which then establishes a genital infection through oral sex — is, in most people’s minds, “not really doing anything wrong.” Someone who discloses a diagnosed genital infection before any contact is treated as if they’re confessing something shameful. The outcomes can be medically identical. The social treatment is entirely different.
For people navigating HSV-1 vs HSV-2 dating, understanding this stigma gap matters for two reasons. First, because it helps you place your own feelings about your diagnosis in their proper context — you are carrying something extraordinarily common, and the shame you may feel was largely constructed by cultural attitudes rather than by the actual significance of the infection. Second, because when you’re in the disclosure conversation, you’re not just sharing a medical fact — you’re navigating someone else’s stigma, which may have nothing to do with what the research actually shows.
Does Your HSV Type Change How — or Whether — You Disclose?
Legally, no. In the United States and Canada, both HSV-1 and HSV-2 fall under the same STI disclosure frameworks. Whether you have genital herpes in Florida, New York, or are dating in Canada, the legal obligation to disclose an STI before sex applies to both types. Having genital HSV-1 does not exempt you from this.
Practically, though, your HSV type does shape the content of the conversation — and can make it somewhat easier with genital HSV-1.
Disclosing Genital HSV-1
Because most people already understand that oral HSV-1 is extremely common, you can ground the conversation in something familiar: “Most people already carry HSV-1 orally — mine is the same virus, acquired genitally. It tends to recur rarely after the first year, and the shedding rate is much lower than HSV-2. Here’s what that means for us…”
This framing isn’t spin — it’s accurate. And accuracy, delivered calmly, is generally the most effective way to navigate this conversation.
Disclosing Genital HSV-2
With HSV-2, the conversation requires more context, particularly around transmission risk. Being able to say you’re on suppressive therapy — which reduces HSV-2 transmission risk by approximately 48% in discordant couples (CDC STI Treatment Guidelines) — gives your partner something concrete to hold onto. So does being specific about your outbreak pattern, how long you’ve had the infection, and how you manage it day to day.
Both conversations are manageable. The people who navigate them best are generally those who know their own type, understand the data, and approach the discussion as information-sharing rather than confession.
The Disclosure Toolkit: What to Say and When to Say It
One of the biggest hurdles in dating with HSV is the “Talk.” But disclosure doesn’t have to be a confession of a crime—it’s simply sharing a medical detail out of respect for your partner. Here are three proven scripts to help you navigate the conversation.
Strategy A: The “Common Ground” Approach (Best for Genital HSV-1)
Why it works: It leverages the fact that most people are already familiar with oral cold sores.
“Before things get more intimate, I want to be upfront about something. I carry the HSV-1 virus—it’s the same one that causes common oral cold sores in about 60% of people. In my case, however, the infection is genital.
The Key Point: Because this virus prefers the mouth area, it’s very ‘out of its element’ downstairs. It rarely recurs and the transmission risk is significantly lower than typical genital herpes (HSV-2). I’m telling you because I value our trust. Have you ever been tested for HSV-1?”
Strategy B: The “Data-Driven” Approach (Best for Genital HSV-2)
Why it works: It uses logic and safety measures to lower the perceived risk.
“I’m really enjoying where this is going. Because I care about your health, I wanted to share that I have HSV-2.
The Key Point: While that might sound a bit heavy, I manage it proactively. I take daily suppressive medication, which cuts the transmission risk by about half. When we use condoms and avoid sex during any rare flare-ups, the actual risk of you catching it is less than 1% per year. It’s just a minor skin condition to me. Do you have any questions about how it works?”
Strategy C: The “Normalized” Approach (Best for Casual or Confident Vibes)
Why it works: It treats the diagnosis as a minor detail, which helps the partner stay calm.
“Hey, before we take the next step, I have a quick ‘health update’ for us. I carry HSV (Herpes). It sounds like a big deal because of the stigma, but it’s actually something billions of people live with.
The Key Point: I’ve got my routine down with [meds/protection] to keep everything safe. For me, it’s just a small physical detail, like having an allergy. I wanted to give you the choice and see how you feel about it.”
Suppressive Therapy: Does Your HSV Type Affect Whether You Need It?
Yes, and this is one of the most practical differences between the two types for people who are actively dating.
HSV-2: Generally Recommended
For people with genital HSV-2, daily suppressive therapy — typically valacyclovir — is broadly recommended by clinical guidelines, including the CDC’s STI Treatment Guidelines. The reasons are clear: HSV-2 maintains high shedding rates for years, and suppressive therapy reduces recurrence frequency by 70–80%, reduces shedding by 80–95%, and reduces transmission risk to an HSV-negative partner by approximately 48%. For anyone in a relationship with an HSV-negative partner, the case for daily suppressive therapy is strong.
Genital HSV-1: Context-Dependent
Because genital HSV-1 recurs infrequently and shedding declines rapidly after the first year, daily suppressive therapy is not routinely recommended for most people with genital HSV-1. The exception is the first year of infection — when shedding rates are at their peak — and situations where an HSV-1-positive person is in a relationship with an HSV-negative partner who wants the additional protection suppressive therapy provides.
Your doctor is the right person to have this conversation with. The point here is simply that your type genuinely does affect the clinical recommendation — and if you’ve been told “you need daily antivirals” without your type being taken into account, it may be worth revisiting that advice.
The Layered Defense: Exactly How Much Can You Reduce Risk?
Relying on one method is good; stacking them is better. Based on clinical data from sources like the New England Journal of Medicine, here is how “layered defense” drastically changes the transmission math:
Suppressive Therapy (Daily Meds): Reduces the risk of transmission to a partner by approximately 48%.
Condoms: A powerful barrier, though the protection level varies by gender:
Male-to-Female: Reduces risk by ~96% (as most shedding areas are covered).
Female-to-Male: Reduces risk by ~65% (due to wider shedding areas).
The Power of Both: When you combine daily antivirals with consistent condom use—and avoid sex during outbreaks—the annual transmission risk for HSV-2 in discordant couples drops to less than 1%.
Side-by-Side: HSV-1 vs HSV-2 Dating
The table below summarises the key differences in the dimensions that matter most when you’re dating with herpes. It is designed as a reference — not as a statement that one type is “better” than the other, but because having accurate information is the foundation of every good disclosure conversation.
| Factor | Genital HSV-1 | Genital HSV-2 |
|---|---|---|
| Global prevalence (genital) | ~376 million (rising ~1–2%/year) | ~520 million (slowly declining) |
| Median annual recurrences | ~1 (declines further over time) | ~5 (persists for years) |
| Asymptomatic shedding — year 1 | ~5% of days | ~33.6% of days |
| Asymptomatic shedding — 10 years | Declines significantly (est. <1–2%) | ~17% of days (remains elevated) |
| Disclosure obligation | Yes — same legal/ethical standard | Yes — same legal/ethical standard |
| Suppressive therapy — routine? | Not routinely; consider in year 1 or discordant couples | Broadly recommended, esp. with HSV-negative partner |
| Transmission reduction with therapy | Limited data; likely similar mechanism | ~48% reduction in acquisition; 75% reduction in symptomatic disease |
| Disclosure conversation framing | Can leverage familiarity with oral HSV-1 | Requires more context; shedding data important |
| Stigma (social) | Lower — but unfairly so | Higher — but unfairly so |
| Prior HSV-1 as protection vs HSV-2? | Partial only — reduces severity of initial HSV-2, not infection risk | |
Sources: Johnston et al., JAMA 2022; WHO / Harfouche et al., STI 2025; Journal of Infection 2025; CDC STI Treatment Guidelines 2021.
Frequently Asked Questions About HSV-1 vs HSV-2 Dating
Is HSV-1 or HSV-2 “worse” for dating?
Neither is objectively worse, but they offer different experiences when navigating the HSV-1 vs HSV-2 dating landscape. Genital HSV-2 typically involves more frequent outbreaks (a median of 5 per year vs. 1 for HSV-1) and maintains higher shedding rates for much longer. This affects daily management and the specific transmission data you share with a partner. Genital HSV-1 tends to recur rarely and becomes significantly less contagious over time. Both require the same level of honesty, and both carry a social stigma that is disproportionate to their actual medical impact.
Is genital HSV-1 less contagious than HSV-2?
Based on current evidence, yes. A landmark 2022 study found that genital HSV-1 sheds on roughly 5% of days in the first year, compared to 33.6% for HSV-2. By year three, HSV-1 shedding often drops to around 1.3%. Lower shedding translates to lower transmission probability. While this is not a reason to skip disclosure, it is highly accurate and reassuring information for your partner to have.
Can you date with genital HSV-1 without telling someone?
No. The specific type of herpes you carry does not change your ethical or legal disclosure obligations. Both HSV-1 and HSV-2 are covered under STI disclosure laws in most U.S. states and in Canada. Whether you have HSV-1 or HSV-2, the requirement to inform a partner before sexual contact remains the same.
Does having HSV-1 protect you from getting HSV-2?
Only partially. A prior HSV-1 infection (like oral cold sores) can reduce the severity of an initial HSV-2 episode if acquired later in life because your immune system is already familiar with the virus family. However, it does not prevent HSV-2 infection, and it does not reduce long-term HSV-2 shedding or recurrence rates.
Do I need suppressive therapy if I have genital HSV-1?
Not automatically. Because genital HSV-1 has low recurrence rates and rapidly declining shedding, daily antiviral therapy is not routinely recommended for most people after the first year. However, it may be considered if you have an HSV-negative partner who wants added peace of mind. Those with HSV-2 generally have a much stronger clinical case for daily suppressive therapy to manage more frequent symptoms.
What’s the best platform for HSV-1 vs HSV-2 dating?
BraveMatchs is specifically designed to support the HSV-1 vs HSV-2 dating community. It serves people with both types (and other STIs) in an environment where disclosure is already a given. Whether you’re navigating the dating scene in Florida, New York, or Toronto, our platform lets you skip the “disclosure anxiety” and focus entirely on finding a real connection with someone who already understands.
The Bottom Line
At the end of the day, HSV-1 vs HSV-2 dating involves navigating two related but genuinely different experiences. Genital HSV-1 tends to recur rarely, sheds at lower rates, and becomes significantly less transmissible over time. In contrast, Genital HSV-2 is more persistent—with more frequent outbreaks, higher shedding rates, and a stronger clinical case for ongoing suppressive therapy.
What doesn’t differ is the ethical foundation of your relationships: both require honest disclosure before sexual contact. Both carry a social stigma that is entirely out of proportion to their actual medical profile.
The most important takeaway for anyone dating with HSV-1 vs HSV-2 is that millions of people are already doing it successfully. They are building deep, healthy, and viral-safe relationships every day—because honest communication, the right medical data, and the right platforms make all the difference.